Скачать с ютуб Acute Renal Failure: How to approach ARF in 4 minutes with Robert Bell M.D. в хорошем качестве
Acute Renal Failure: How to approach ARF in 4 minutes with Robert Bell M.D.
6 лет назад
Скачать бесплатно Acute Renal Failure: How to approach ARF in 4 minutes with Robert Bell M.D. в качестве 4к (2к / 1080p)
У нас вы можете посмотреть бесплатно Acute Renal Failure: How to approach ARF in 4 minutes with Robert Bell M.D. или скачать в максимальном доступном качестве, которое было загружено на ютуб. Для скачивания выберите вариант из формы ниже:
Загрузить музыку / рингтон Acute Renal Failure: How to approach ARF in 4 minutes with Robert Bell M.D. в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса savevideohd.ru
Acute Renal Failure: How to approach ARF in 4 minutes with Robert Bell M.D.
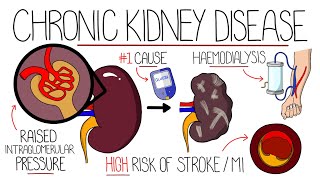
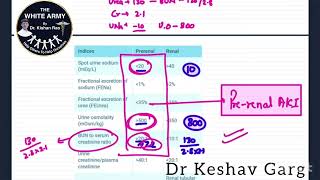
Acute renal failure refers to the sudden and significant reduction of kidney function, as quantified by a reduction in the glomerular filtration rate and elevation of serum creatinine concentration. Commonly occurring in hospitalized patients, rapid assessment and prompt management is crucial to minimize or prevent complications from acute renal failure. medskl.com is a global, free open access medical education (FOAMEd) project covering the fundamentals of clinical medicine with animations, lectures and concise summaries. medskl.com is working with over 170 award-winning medical school professors to provide content in 200+ clinical presentations for use in the classroom and for physician CME. Nephrology - Acute Renal Failure: What you need to know Whiteboard Animation Transcript with Robert Bell, MD https://medskl.com/module/index/acute... What do you do when a serum creatinine value from a patient you see in the ER is elevated? Diagnosis of ARF usually requires an acute rise in serum creatinine representing a fall in GFR, often with a decrease in urine output to less than 500 ml per day (oliguria). First, decide if low GFR is acute or chronic. If no previous data is available to suggest it is chronic, small kidneys seen on ultrasound imaging is strongly suggestive of chronic disease. (Note that normal sized kidneys can be seen with chronic kidney disease). Next, if this is ARF, is it: 1. Pre-renal Decreased renal blood flow, but no structural or functional renal damage. 2. Renal Damage to glomeruli or renal tubules, such as ATN, RPGN, AIN. 3.Post-renal Obstruction of ureters. Workup is focused on the cause: 1. Pre-renal For “ARF” check fractional excretion of sodium (FENa). For oliguric patients, a FENa less than 1% is predictive of pre-renal failure and a FENa greater than 2% is predictive of ATN. *There are many exceptions to this rule. 2. Renal For oliguric ATN check FENa as stated. Don’t forget the possibility of RPGN or AIN, and use the urinalysis to help diagnose these. 3. Post-Renal The finding of bilateral hydronephrosis on ultrasound is highly predictive of post-renal ARF. Management 1. Pre-renal Restoration of effective circulating volume will restore GFR to baseline 2. Renal Treatment for ATN is supportive Avoid nephrotoxins Treatment of RPGN and AIN depends on the results of the workup 3. Post-renal Removing the obstruction will improve GFR; the amount of improvement depends on the duration and severity of the obstruction If the cause of the ARF cannot be easily treated, manage its consequences. Consequences that require urgent dialysis are: A. Acidosis E. Electrolytes (mainly hyperkalemia) I. Intoxicants (i.e methanol, ethylene glycol, Li+, ASA) O. Volume Overload (i.e. pulmonary edema) U. Severe Uremic complications SUMMARY When your patient’s serum creatinine is elevated and represents ARF, following this approach will take you from diagnosis to appropriate management.
Comments